Blank Indiana Sr21 PDF Template
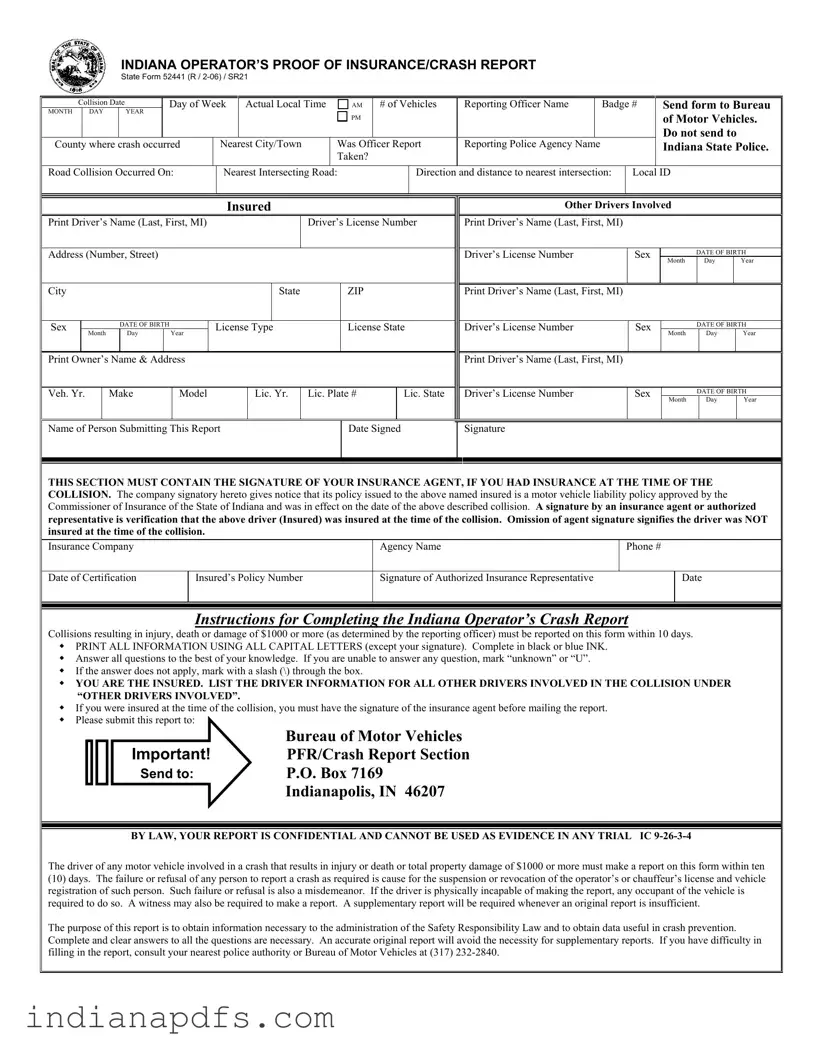
In the aftermath of a motor vehicle collision in Indiana, the SR21 form, officially known as the Operator’s Proof of Insurance/Crash Report, becomes a crucial document for all parties involved. This form must be completed and submitted to the Bureau of Motor Vehicles within ten days of a crash that results in injury, death, or property damage exceeding $1,000. It requires detailed information about the incident, including the date, time, and location of the collision, as well as specifics about the vehicles and drivers involved. Each driver must provide their personal details, such as name, address, and driver's license number, while the report also necessitates the inclusion of the insurance agent's signature if coverage was in place at the time of the incident. The SR21 serves not only as a record of the collision but also plays a vital role in ensuring compliance with Indiana’s Safety Responsibility Law. Failure to submit this report can lead to serious consequences, including the suspension of driving privileges. It is essential that those involved understand the urgency of accurately completing this form to avoid potential legal repercussions and contribute to data collection aimed at improving road safety.
Form Sample
INDIANA OPERATOR’S PROOF OF INSURANCE/CRASH REPORT
STATE FORM 52441 (R /
Collision Date |
|
Day of Week |
Actual Local Time |
AM |
# of Vehicles |
Reporting Officer Name |
|
Badge # |
Send form to Bureau |
||||||
MONTH |
DAY |
|
YEAR |
|
|
|
|
PM |
|
|
|
|
|
|
of Motor Vehicles. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Do not send to |
County where crash occurred |
|
Nearest City/Town |
Was Officer Report |
Reporting Police Agency Name |
|
|
Indiana State Police. |
||||||||
|
|
|
|
|
|
|
|
Taken? |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||
Road Collision Occurred On: |
|
Nearest Intersecting Road: |
|
Direction and distance to nearest intersection: |
Local ID |
||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Insured
Print Driver’s Name (Last, First, MI) |
|
|
|
Driver’s License Number |
||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
Address (Number, Street) |
|
|
|
|
|
|
|
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
City |
|
|
|
|
|
|
State |
|
ZIP |
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
Sex |
|
|
|
DATE OF BIRTH |
|
License Type |
|
License State |
||||
|
Month |
|
Day |
|
Year |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Print Owner’s Name & Address |
|
|
|
|
|
|
||||||
|
|
|
|
|
|
|
|
|
|
|||
Veh. Yr. |
|
Make |
Model |
|
Lic. Yr. |
Lic. Plate # |
Lic. State |
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
Other Drivers Involved
Print Driver’s Name (Last, First, MI)
Driver’s License Number |
Sex |
|
DATE OF BIRTH |
|
|
|
Month |
Day |
Year |
|
|
|
|
|
Print Driver’s Name (Last, First, MI) |
|
|
|
|
|
|
|
|
|
Driver’s License Number |
Sex |
|
DATE OF BIRTH |
|
|
|
Month |
Day |
Year |
|
|
|
|
|
Print Driver’s Name (Last, First, MI) |
|
|
|
|
|
|
|
|
|
Driver’s License Number |
Sex |
|
DATE OF BIRTH |
|
|
|
Month |
Day |
Year |
|
|
|
|
|
Name of Person Submitting This Report
Date Signed
Signature
THIS SECTION MUST CONTAIN THE SIGNATURE OF YOUR INSURANCE AGENT, IF YOU HAD INSURANCE AT THE TIME OF THE COLLISION. The company signatory hereto gives notice that its policy issued to the above named insured is a motor vehicle liability policy approved by the Commissioner of Insurance of the State of Indiana and was in effect on the date of the above described collision. A signature by an insurance agent or authorized representative is verification that the above driver (Insured) was insured at the time of the collision. Omission of agent signature signifies the driver was NOT insured at the time of the collision.
Insurance Company
Agency Name
Phone #
Date of Certification
Insured’s Policy Number
Signature of Authorized Insurance Representative
Date
Instructions for Completing the Indiana Operator’s Crash Report
Collisions resulting in injury, death or damage of $1000 or more (as determined by the reporting officer) must be reported on this form within 10 days. PRINT ALL INFORMATION USING ALL CAPITAL LETTERS (except your signature). Complete in black or blue INK.
Answer all questions to the best of your knowledge. If you are unable to answer any question, mark “unknown” or “U”. If the answer does not apply, mark with a slash (\) through the box.
YOU ARE THE INSURED. LIST THE DRIVER INFORMATION FOR ALL OTHER DRIVERS INVOLVED IN THE COLLISION UNDER “OTHER DRIVERS INVOLVED”.
If you were insured at the time of the collision, you must have the signature of the insurance agent before mailing the report.
Please submit this report to:
Bureau of Motor Vehicles
Important! PFR/Crash Report Section
Send to: P.O. Box 7169
Indianapolis, IN 46207
BY LAW, YOUR REPORT IS CONFIDENTIAL AND CANNOT BE USED AS EVIDENCE IN ANY TRIAL IC
The driver of any motor vehicle involved in a crash that results in injury or death or total property damage of $1000 or more must make a report on this form within ten
(10)days. The failure or refusal of any person to report a crash as required is cause for the suspension or revocation of the operator’s or chauffeur’s license and vehicle registration of such person. Such failure or refusal is also a misdemeanor. If the driver is physically incapable of making the report, any occupant of the vehicle is required to do so. A witness may also be required to make a report. A supplementary report will be required whenever an original report is insufficient.
The purpose of this report is to obtain information necessary to the administration of the Safety Responsibility Law and to obtain data useful in crash prevention. Complete and clear answers to all the questions are necessary. An accurate original report will avoid the necessity for supplementary reports. If you have difficulty in filling in the report, consult your nearest police authority or Bureau of Motor Vehicles at (317)
Form Specifics
| Fact Name | Fact Description |
|---|---|
| Purpose | The Indiana SR21 form is used to report motor vehicle collisions that result in injury, death, or property damage exceeding $1,000. |
| Filing Deadline | Drivers must submit the SR21 form within 10 days of the collision to comply with Indiana law. |
| Insurance Verification | A signature from the insurance agent is required if the driver had insurance at the time of the crash, confirming the policy was active. |
| Confidentiality | Reports filed using the SR21 form are confidential and cannot be used as evidence in court, as stated in Indiana Code IC 9-26-3-4. |
| Legal Consequences | Failure to file the SR21 form as required can lead to suspension or revocation of the driver's license and vehicle registration. |
Fill out Popular Templates
Eviction Process Indiana - A preparatory document for landlords, setting the foundation for a legal request to repossess properties under specific rental dispute conditions.
To enhance your professional presentation, consider utilizing a customized Recommendation Letter tool that simplifies the process of obtaining valuable endorsements from peers or mentors.
Indiana State 50181 - The form allows for the filing against both organizations and individual debtors, with specific sections dedicated to each.
Indiana Wh 4 - Seasonal workers in Indiana also need to complete a WH-4 form, which can influence their tax withholdings and reflect their unique employment situation.