Blank Indiana Otp 901 PDF Template
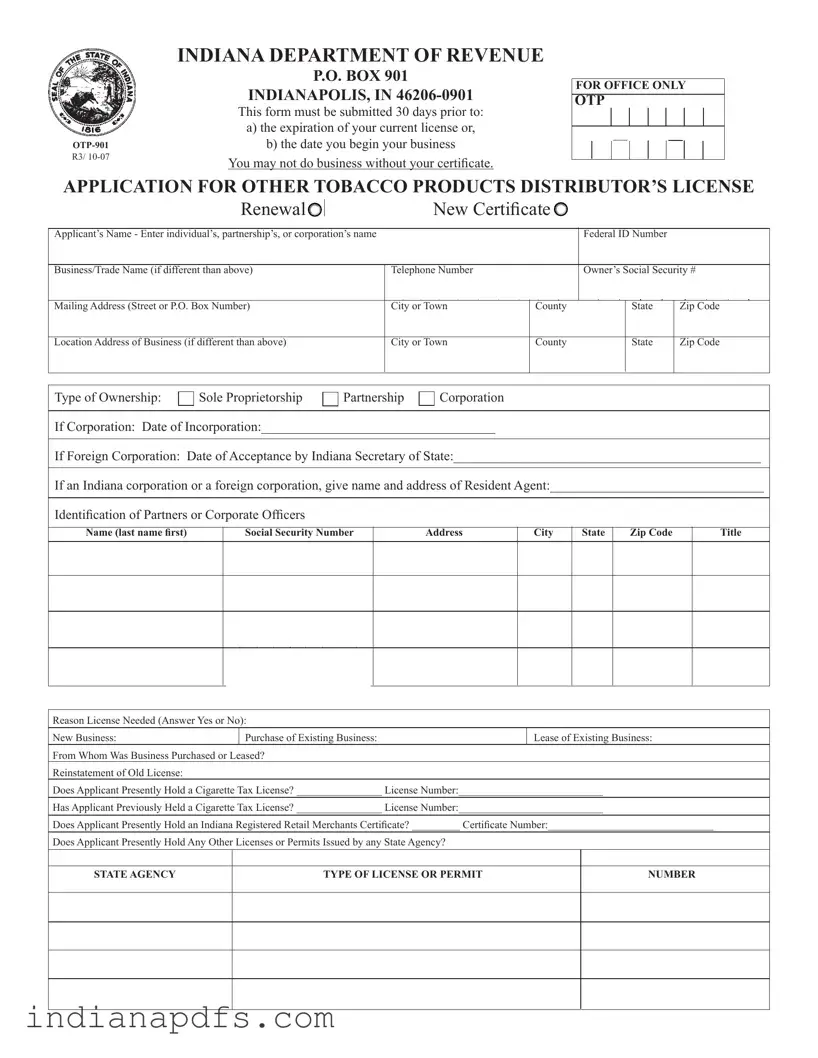
The Indiana OTP 901 form is an essential document for individuals or businesses looking to distribute other tobacco products within the state. This form must be submitted at least 30 days before either the expiration of your current license or the commencement of your business activities. It is crucial to understand that operating without the appropriate certificate is not permitted. The OTP 901 form gathers important information, including the applicant's name, business details, and ownership structure. It also requires disclosure of any existing licenses, such as a cigarette tax license or a retail merchant certificate. Furthermore, applicants must provide details about their business location, partners, and corporate officers, along with any audit information necessary for compliance. The form also asks about anticipated purchases and sales of tobacco products, including any out-of-state transactions. Completing this application accurately and submitting it on time is vital to ensure compliance with Indiana's regulations and to facilitate the smooth operation of your tobacco distribution business.
Form Sample
INDIANA DEPARTMENT OF REVENUE
R3/
P.O. BOX 901
INDIANAPOLIS, IN
This form must be submitted 30 days prior to:
a)the expiration of your current license or,
b)the date you begin your business
You may not do business without your certificate.
FOR OFFICE ONLY
OTP
APPLICATION FOR OTHER TOBACCO PRODUCTS DISTRIBUTOR’S LICENSE
|
|
Renewal |
|
|
|
|
New Certificate |
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Applicant’s Name - Enter individual’s, partnership’s, or corporation’s name |
|
|
|
|
|
|
Federal ID Number |
|
|
|
||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Business/Trade Name (if different than above) |
|
|
|
Telephone Number |
|
|
|
Owner’s Social Security # |
||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Mailing Address (Street or P.O. Box Number) |
|
|
|
City or Town |
County |
|
|
State |
Zip Code |
|||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Location Address of Business (if different than above) |
|
|
|
City or Town |
County |
|
|
State |
Zip Code |
|||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Type of Ownership: |
|
Sole Proprietorship |
|
|
Partnership |
|
Corporation |
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
If Corporation: Date of Incorporation:___________________________________
If Foreign Corporation: Date of Acceptance by Indiana Secretary of State:______________________________________________
If an Indiana corporation or a foreign corporation, give name and address of Resident Agent:________________________________
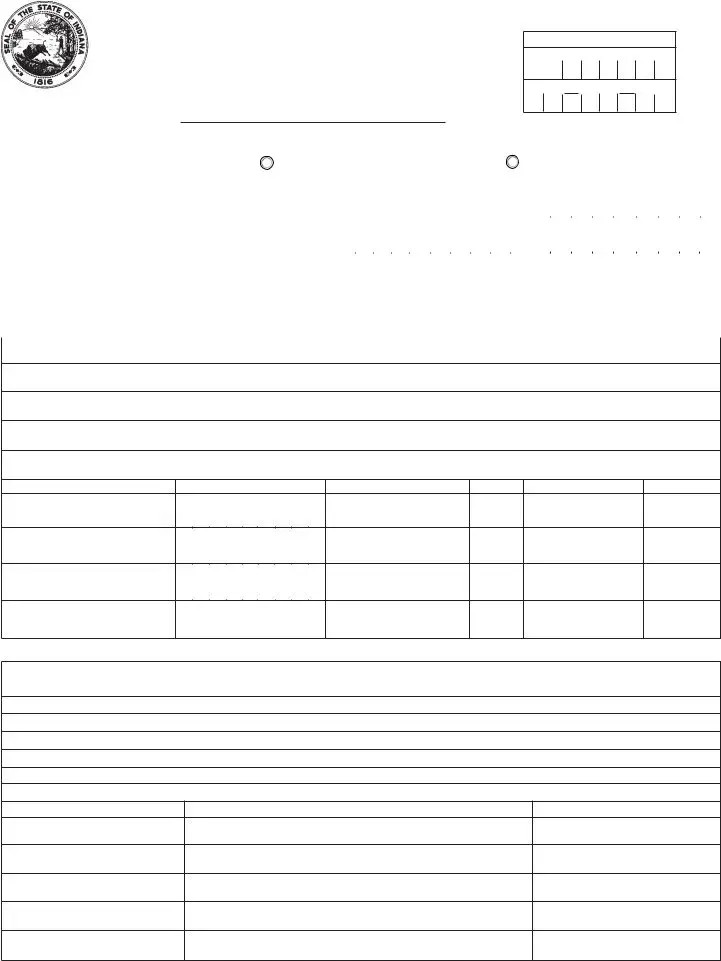
Identifi cation of Partners or Corporate Officers
Name (last name fi rst)
Social Security Number
Address
City
State |
Zip Code |
|
|
Title
Reason License Needed (Answer Yes or No):
New Business: |
Purchase of Existing Business: |
Lease of Existing Business: |
From Whom Was Business Purchased or Leased?
Reinstatement of Old License:
Does Applicant Presently Hold a Cigarette Tax License? ________________ License Number:___________________________
Has Applicant Previously Held a Cigarette Tax License? ________________ License Number:___________________________
Does Applicant Presently Hold an Indiana Registered Retail Merchants Certifi cate? _________ Certificate Number:_______________________________
Does Applicant Presently Hold Any Other Licenses or Permits Issued by any State Agency?
STATE AGENCY
TYPE OF LICENSE OR PERMIT
NUMBER
Audit Information:
Location Where Records Will Be Available For Audit:
Phone Number of Location Of Audit Records:
Phone Number of Business Location:
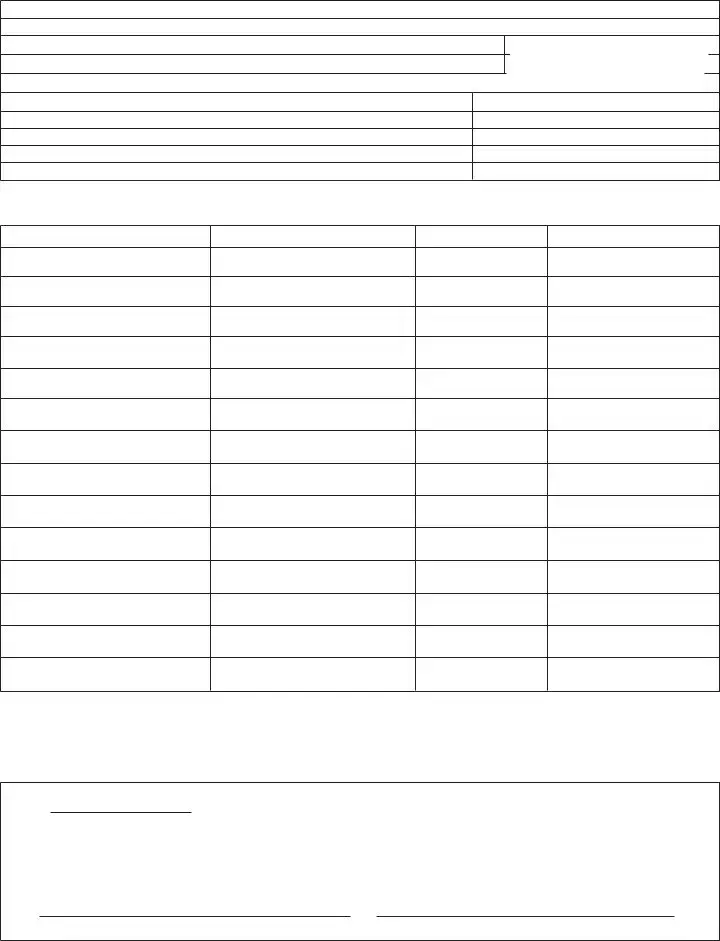
Indicate Address of Each Location In Which You Have Other Tobacco Products in Storage
Location
OTP License Number
Indicate Name, Address, Phone Number and Estimated Annual Purchases from Whom You Currently Purchase and/or Expect to Purchase Other Tobacco Products: (A Computer Generated List Which Includes All Requested Information Will Be Accepted)
Supplier’s Name
Address
Phone Number
Estimated Annual Purchases
TOTAL:
If Necessary Attach Additional List.
Does Your Company Expect to Sell Other Tobacco Products Into Another State?___________________________________________________________________
List States: _________________________________________________________________________________________________________________________
Today’s Date
I declare under penalties of perjury that the information contained in this application and any attachments is true, correct and complete to the best of my knowledge and belief.
Signature of Taxpayer or Authorized Agent, Title |
Telephone Number |
Form Specifics
| Fact Name | Description |
|---|---|
| Form Purpose | The OTP-901 form is used to apply for a distributor's license for other tobacco products in Indiana. |
| Submission Deadline | This form must be submitted 30 days prior to the expiration of your current license or the start date of your business. |
| Governing Law | The Indiana Code Title 6, Article 7, governs the licensing of tobacco product distributors. |
| License Requirement | Applicants cannot conduct business without obtaining a valid distributor's certificate. |
| Types of Ownership | The form accommodates various ownership structures, including sole proprietorships, partnerships, and corporations. |
| Federal ID Number | Applicants must provide their Federal ID number, which is essential for tax purposes. |
| Audit Information | Applicants must indicate where their records will be available for audit, ensuring transparency and compliance. |
| Renewal Options | The form allows for both new applications and renewals of existing licenses, accommodating different business needs. |
| Contact Information | Applicants must provide contact details, including phone numbers for both the business and the audit location. |
| Penalties for False Information | Signing the form includes a declaration under penalties of perjury, emphasizing the importance of accuracy in the information provided. |
Fill out Popular Templates
Daycares Near Me That Take Vouchers - Allows Indiana families to explore financial assistance options for childcare needs.
The Arizona University Application form is a crucial document for students seeking undergraduate admission to Arizona State University, Northern Arizona University, or the University of Arizona. It includes a request for a waiver of the application fee for Arizona residents facing financial hardship. For more information, you can visit https://arizonapdfforms.com/arizona-university-application/. Understanding this form and its requirements is essential for a smooth application process.
Establishing Paternity in Indiana - Addresses the legal aspect of fatherhood in Indiana, paving the way for a more involved and responsible parental role.